Article Text

Abstract
Objective To assess the feasibility of collecting, examining and reporting observational, real-world evidence regarding the novel use of the GORE EXCLUDER Iliac Branch Endoprosthesis (IBE) in conjunction with the GORE VIABAHN VBX Balloon Expandable Endoprosthesis (IBE+VBX stent graft).
Design Multicentre retrospective cohort study.
Setting Four real-world data sources were used: a national quality improvement registry, a statewide clinical research network, a regional quaternary health system and two tertiary academic medical centres.
Participants In total, 30 patients with 37 IBE+VBX stent graft were identified. Of those, the mean age was 72±10.2 years and 90% were male. The cohort was 77% white, 10% black, 3% Hispanic and 10% other.
Main outcome measures Outcome measures included: proportion of percutaneous vs open surgical access, intensive care admission, intensive care unit (ICU) length-of-stay (LOS), total LOS, postoperative complications, discharge disposition and 30-day mortality.
Results The majority (89%) of cases were performed percutaneously, 5% required surgical exposure following failed percutaneous access and 6% required open surgical exposure outright. Nearly half (43%) required intensive care admission with a median ICU LOS of 1 day (range: 1–2). Median total LOS was 1 day (IQR: 1–2). There were zero postoperative myocardial infarctions, zero reported leg embolisations and no reported reinterventions. Access site complications were described in 1 of 28 patients, manifesting as a haematoma or pseudoaneurysm. Ultimately, 97% were discharged to home and one patient was discharged to a nursing home or rehabilitation facility. There were no 30-day perioperative deaths.
Conclusions This project demonstrates the feasibility of identifying and integrating real-world evidence, as it pertains to an unapproved combination of endovascular devices (IBE+VBX stent graft), for short-term outcomes analysis. This new paradigm of evidence has potential to be used for device monitoring, submission to regulatory agencies, or consideration in indication expansions and approvals with further efforts to systematise data collection and transmission mechanisms.
- Real World Evidence
- Vascular Devices
- Device Approval
Data availability statement
No data are available. Data contains PHI and is governed by bilateral data sharing agreements between the Coordinating Center Site and Duke and OneFlorida, and pre-existing agreements with the Society for Vascular Surgery Patient Safety Organisation, and AHRQ listed patient safety organisation. Due to the small sample size, data can not be shared.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In the USA, the GORE EXCLUDER Iliac Branch Endoprosthesis (IBE) has been approved by the Food and Drug Administration for the endovascular treatment of common iliac artery aneurysms, but catheter-based placement of the internal iliac artery branch device can be difficult under certain anatomical circumstances. Registries and other real-world data sources have documented off-label use of the GORE VIABAHN VBX Balloon Expandable Endoprosthesis in conjunction with the GORE EXCLUDER IBE.
What are the new findings?
This study demonstrates the feasibility of using real world evidence to assess the novel use of the GORE EXCLUDER IBE in conjunction with the GORE VIABAHN VBX Balloon Expandable Endoprosthesis (IBE+VBX stent graft). Thirty patients with 37 IBE+VBX stent graft were identified and key intraoperative and postoperative outcomes at the patient level were evaluated.
How might these results affect future research or surgical practice?
This new paradigm of evidence has the potential to be used for device monitoring, submission to regulatory agencies, or consideration in indication expansions and approvals with further efforts to systematise data collection and transmission mechanisms.
Introduction
Endovascular repair of common iliac artery (CIA) aneurysms has been the focus of recent advancements. In the United States (US), the GORE EXCLUDER Iliac Branch Endoprosthesis (IBE; W. L. Gore & Associates, Flagstaff, AZ) was approved by the Food and Drug Administration (FDA) in 2016 for the endovascular treatment of CIA aneurysms or aortoiliac aneurysms.1 The IBE device is comprised of two components: a main body implanted in the CIA and an internal iliac stent graft component (IIC) that extends into the internal iliac artery (IIA).
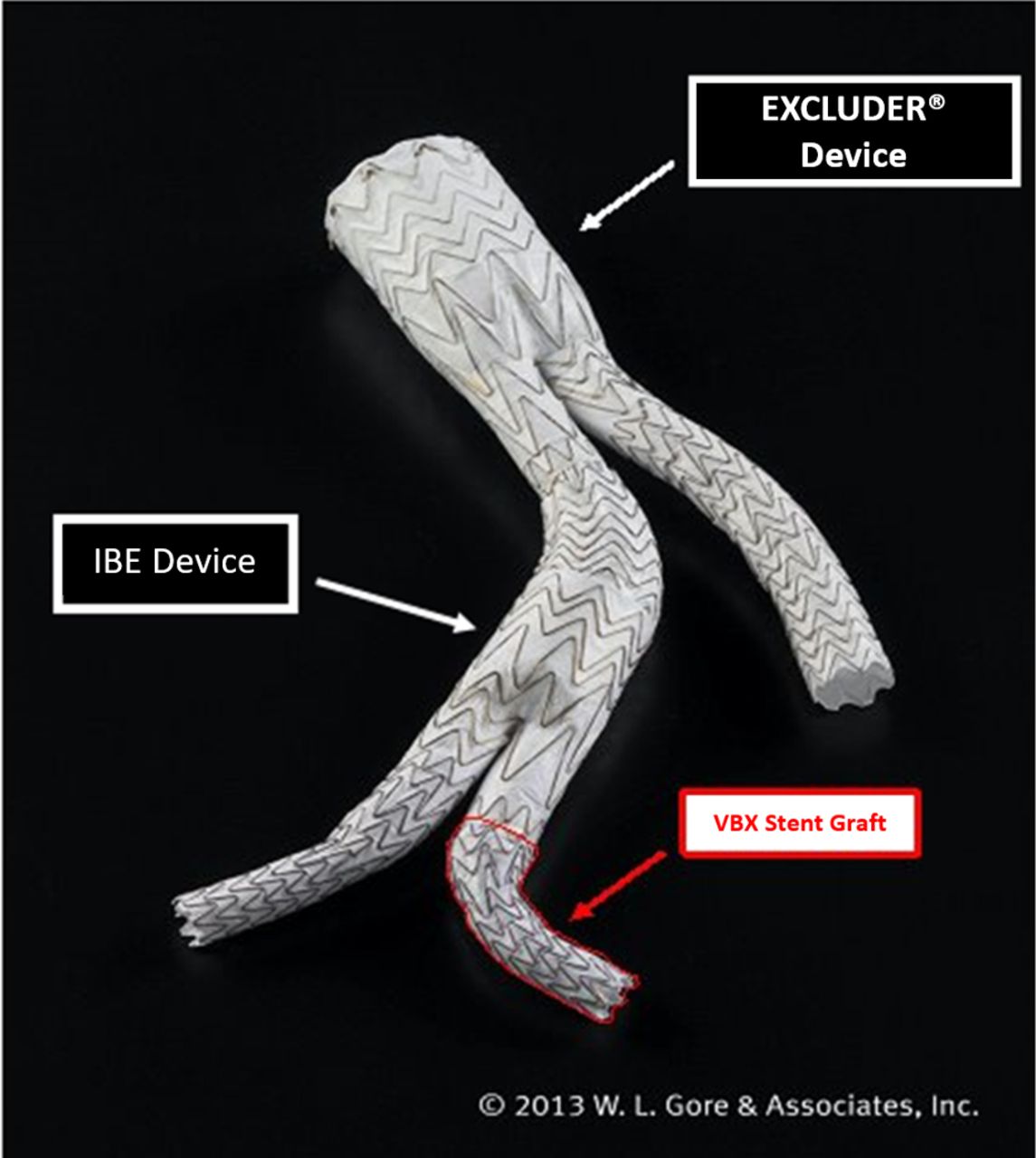
However, catheter-based placement of the IIA branch device can be difficult, especially when the anatomy is tortuous. The Global Registry for Endovascular Aortic Treatment (GREAT Registry) has demonstrated that physicians are willing to use other commercially available products with the IBE device in lieu of the IIC should anatomical circumstances, such as excessive tortuosity, warrant a more flexible device.2 Of 92 patients treated with the IBE device in the GREAT Registry, 6 (7%) did not have the IIC implanted.2 Published case reports have described the utilisation of the GORE VIABAHN VBX Balloon Expandable Endoprosthesis (VBX stent graft), specifically, in conjunction with or in lieu of the IIC (figure 1).3 4 The VBX stent graft device and its delivery system have greater trackability across tortuous anatomy and longer shaft length which permits delivery from upper extremity brachial artery access. The real-world utilisation frequency and performance outcomes of these off-label substitutions outside the GREAT Registry are not well defined.
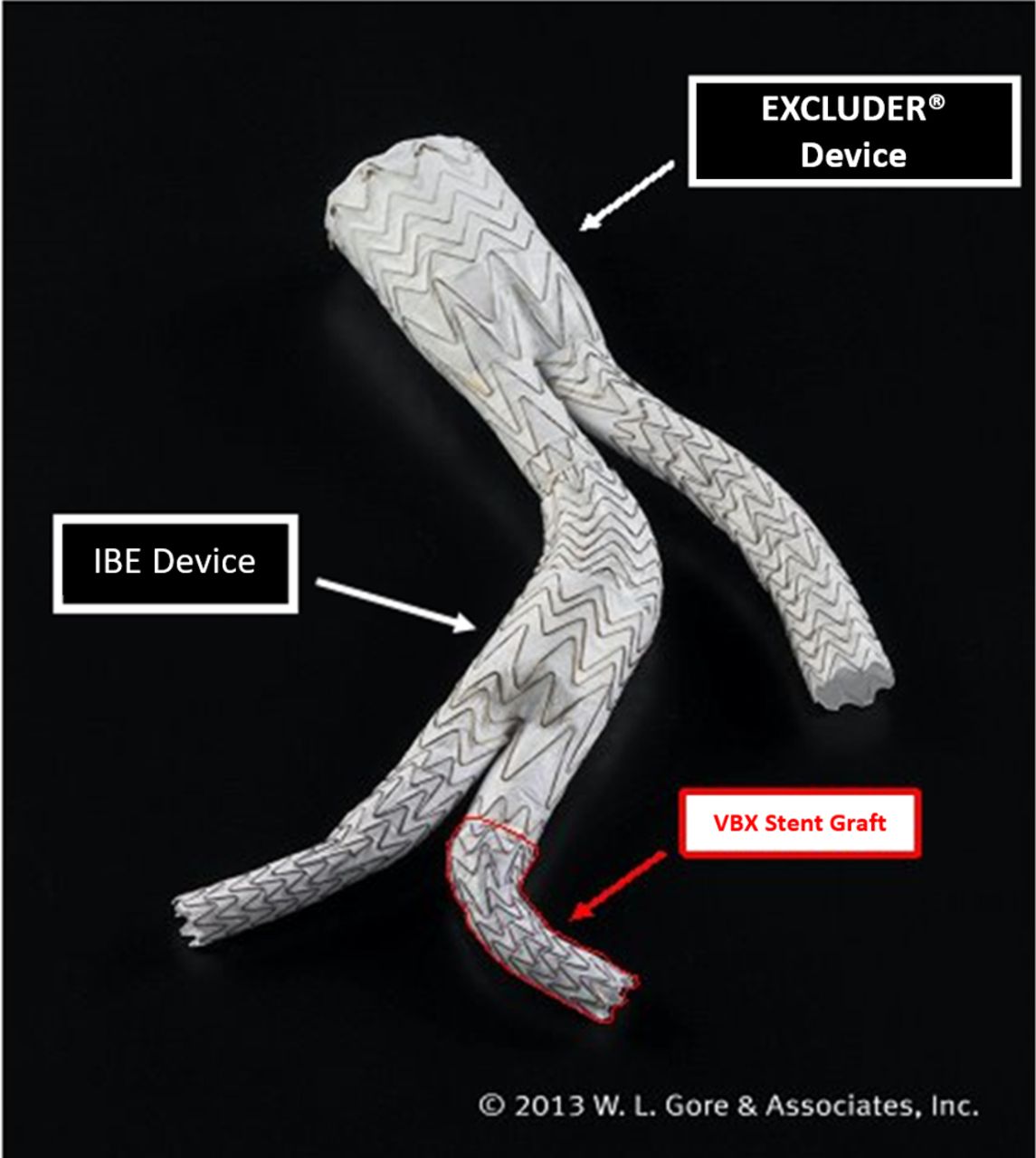
Example image of GORE EXCLUDER Iliac Branch Endoprosthesis (IBE) depicting location of studied GORE VIABAHN VBX balloon expandable endoprosthesis (VBX stent graft) device (note: the on-label internal iliac component is used in this image).
For this reason, we sought to evaluate the feasibility of collecting and examining observational, real-world and registry-derived evidence regarding the novel placement of a GORE EXCLUDER IBE with a substitution of the internal iliac branch component with a GORE VIABAHN VBX Balloon Expandable Endoprosthesis, termed IBE+VBX stent graft. We also sought to evaluate the feasibility of assessing and reporting on the short-term outcomes collected pertaining to this off-label use of existing IBE and VBX stent graft endografts.
Methods
Data sources
This project used four distinct data sources: a national quality improvement registry (the Vascular Quality Initiative (VQI), www.vqi.org), a statewide clinical research network (OneFlorida, www.onefloridaconsortium.org), a regional quaternary health system (DukeHealth, www.dukehealth.org) and tertiary academic medical centres (Dartmouth-Hitchcock Medical Center, https://www.dartmouth-hitchcock.org and Weill Cornell Medicine, https://weillcornell.org/).
The VQI is a collaborative of regional quality groups that collect perioperative and 1 year follow-up data, beginning in 2003, to generate real-time benchmarked quality reports in vascular surgery.5 The VQI is governed by the Society for Vascular Surgery Patient Safety Organisation (SVS-PSO), which provides oversight of data sharing arrangements, key outcome and quality measure analyses, and dissemination of information to participating providers. Given this, the VQI was well suited to serve as a data source in which cases could be identified.
The participating organisations were selected in order to compile an array of organisations in terms of size and structure. The OneFlorida Clinical Research Consortium and its partners provide care for approximately 50% of the patient population in the nation’s third largest state, Florida. Through their centralised OneFlorida Data Trust infrastructure, case identification and data collection could be performed across partner sites. Similarly, Duke Health encompasses several hospitals across the state of North Carolina and allowed for case identification and data collection across the health system.
Dartmouth-Hitchcock Medical Center and Weill Cornell Medicine were also included as participating sites because both clinical centres have an active endovascular branched aortic treatment programme. Further, both sites have robust research enterprises in conjunction with their clinical practices. This allowed for facile case identification and data collection at both sites. Lastly, these sites both participate in the VQI, which allowed for utilisation of the VQI’s secure, HIPAA-compliant cloud-based Pathways programme for secure data transfer.6
Case identification
Initial case identification feasibility was ascertained through de-identified monthly IBE device use records which Gore provided to each site. These records were meant to provide a monthly approximation of overall IBE device procedural volume but was not specific to IBE+VBX stent graft. This data did not include any Personal Health Information or any information that could be traced back to a treated subject. Case identification methods were then devised internally at each study site and underwent site-specific approval. As a result, case identification methods varied across participating sites (table 1). Each case was confirmed through local chart review in which the implantation of the IBE and VBX stent graft device components together was verified. Any potential case in which either the IBE or VBX stent graft device component was not implanted, or the components were implanted but not in conjunction with one another, was excluded.
Case identification and confirmation strategies across participating study sites and the Vascular Quality Initiative (VQI)
Case identification within the VQI registry itself was performed through a records query on the search terms ‘Device’=Gore, and ‘iliac distal endpoint’=external and internal (branched) of all records from 2003 to 2019. Following this rudimentary case identification, cases were confirmed through the documentation of ipsilateral IBE and VBX stent graft device implantation in the IIA. The study team then coordinated with the SVS-PSO who contacted the surgeons associated with all confirmed cases within VQI. Each was asked to use the hashtag variables to supplement the information within VQI. Up to three follow-up requests were sent requesting this information. Only cases for which the hashtag variables were entered into VQI were included for analysis and all others were excluded.
Outcome measures
We evaluated intraoperative and postoperative outcomes at the patient level. Intraoperative outcomes included the proportion of cases performed with percutaneous versus open surgical access, intravenous contrast administration, fluoroscopy time, and reported intraoperative complications. Postoperative outcomes included admission to the intensive care unit (ICU), ICU length-of-stay (LOS), total LOS, postoperative complications, in-hospital reintervention, change in serum creatinine, discharge disposition and 30-day mortality.
Case report form generation
A detailed case report form (CRF) was generated, which allowed for assessment of patient, aneurysm, and procedural characteristics (online supplemental appendix 1). The variables in the CRF were based on the definitions used in the Vascular Quality Initiative Endovascular Aortic Repair (EVR) module.7 The CRF fields and definitions directly mirrored those within the VQI and were used to collect data for cases not eligible for inclusion in the VQI at each site. VQI inclusion criteria are listed in online supplemental appendix 2. Use of local CRF databases allowed for seamless data collection and eventual aggregation with VQI data, while preserving the individual data security at each site.
Supplemental material
Supplemental material
Hashtag variable generation
Given the specific focus of this work, we sought to identify additional information that was not part of the standardised EVR VQI data entry process that would allow for case identification and device specifications. To do this, we used an innovative process which allowed additional variables specific to IBE+VBX stent graft cases to be added into the VQI registry. This process leveraged an existing system developed by the VQI to allow researchers to add new, temporary variables to the registry without the cost and time delay associated with modifying the data input forms in VQI Pathways. This system uses the concept of hashtags (#) to separate and identify new, discrete variables, which can be entered into the existing comments section of each data form. These variables are termed hashtag (#) variables. An instructional guide and standardised set of hashtag variables which captured the IBE+VBX stent graft data of interest were created, tested and approved by the VQI (table 2). These variables were similarly included in the CRF to ensure the VQI and CRF database data could be seamlessly combined.
Hashtag variables designed to capture IBE+VBX specific information and supplement data within the Vascular Quality Initiative (VQI)
Data transfer and aggregation
Weill Cornell Medicine was designated as the coordinating centre site. Therefore, all data were compiled at each local site and then transferred to Cornell for aggregation. Patients with IBE+VBX stent graft identified at VQI-participating study sites (Dartmouth-Hitchcock Medical Center and Weill Cornell Medicine) who met inclusion criteria for the VQI registry were entered into VQI in the normal fashion with the addition of the hashtag variables. As a participating VQI site, Cornell was able to request a deidentified dataset containing all cases with the specified hashtag variables from VQI.
Data from patients who did not meet VQI inclusion criteria (online supplemental appendix 2) or were identified at non-VQI study sites (Duke Health and OneFlorida) were entered into the CRF database locally at each centre. Mirroring data use agreements (DUAs) were established between each site and the coordinating centre at Weill Cornell Medicine. Once in place and at the conclusion of case identification, the CRF databases were transferred for aggregation at the coordinating centre site via secure file transfer protocols.
Statistical analysis
Results from descriptive analysis were presented as means with SD for continuous variables, and percentages for categorical variables. All analyses were performed using SAS V.9.4 (SAS Institute).
Patient and public involvement
This research was conducted without patient involvement. Patients were not involved in the study design or interpretation of the results. Patients did not contribute to the writing or editing of this document.
Results
Cohort identification and sources
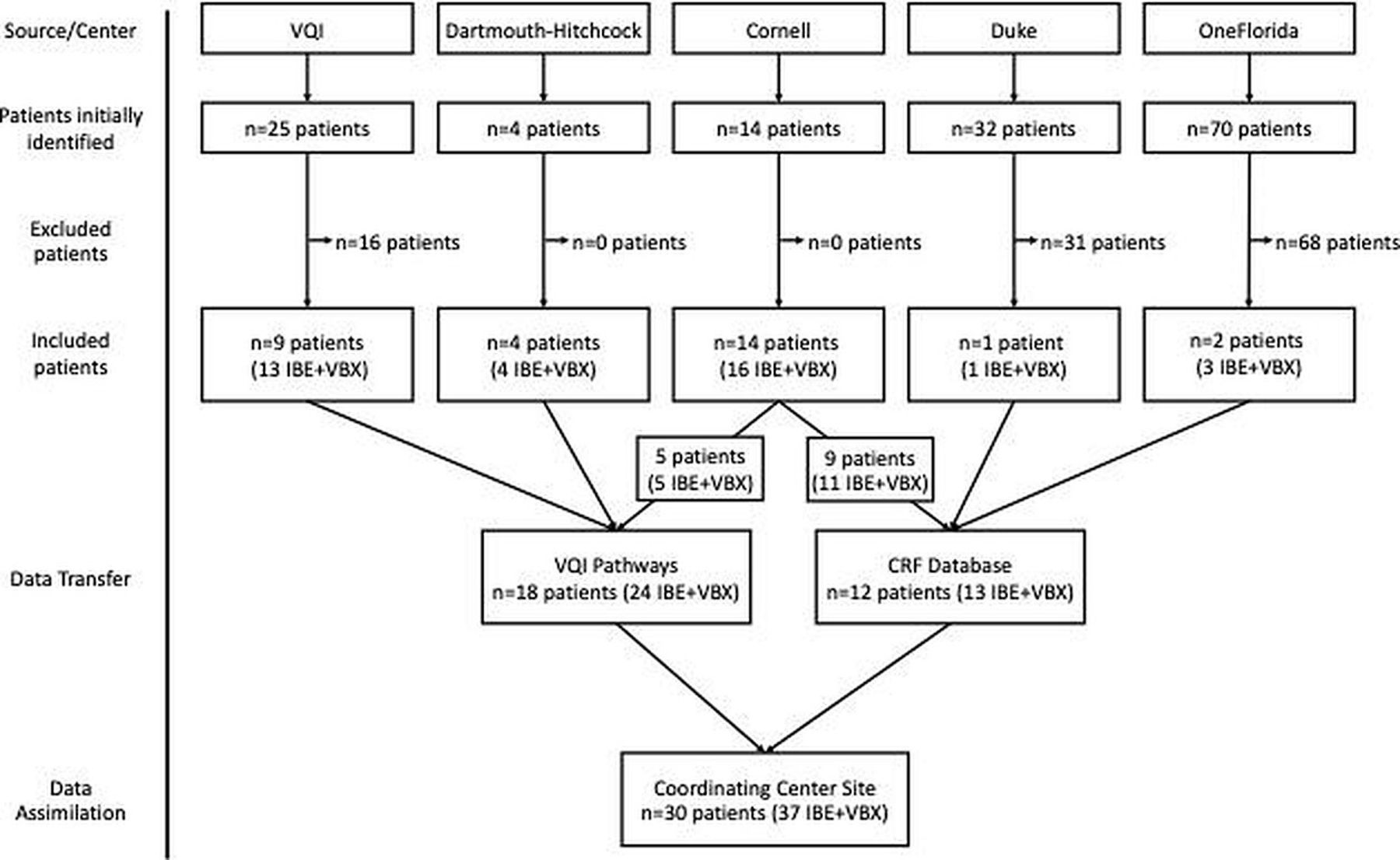
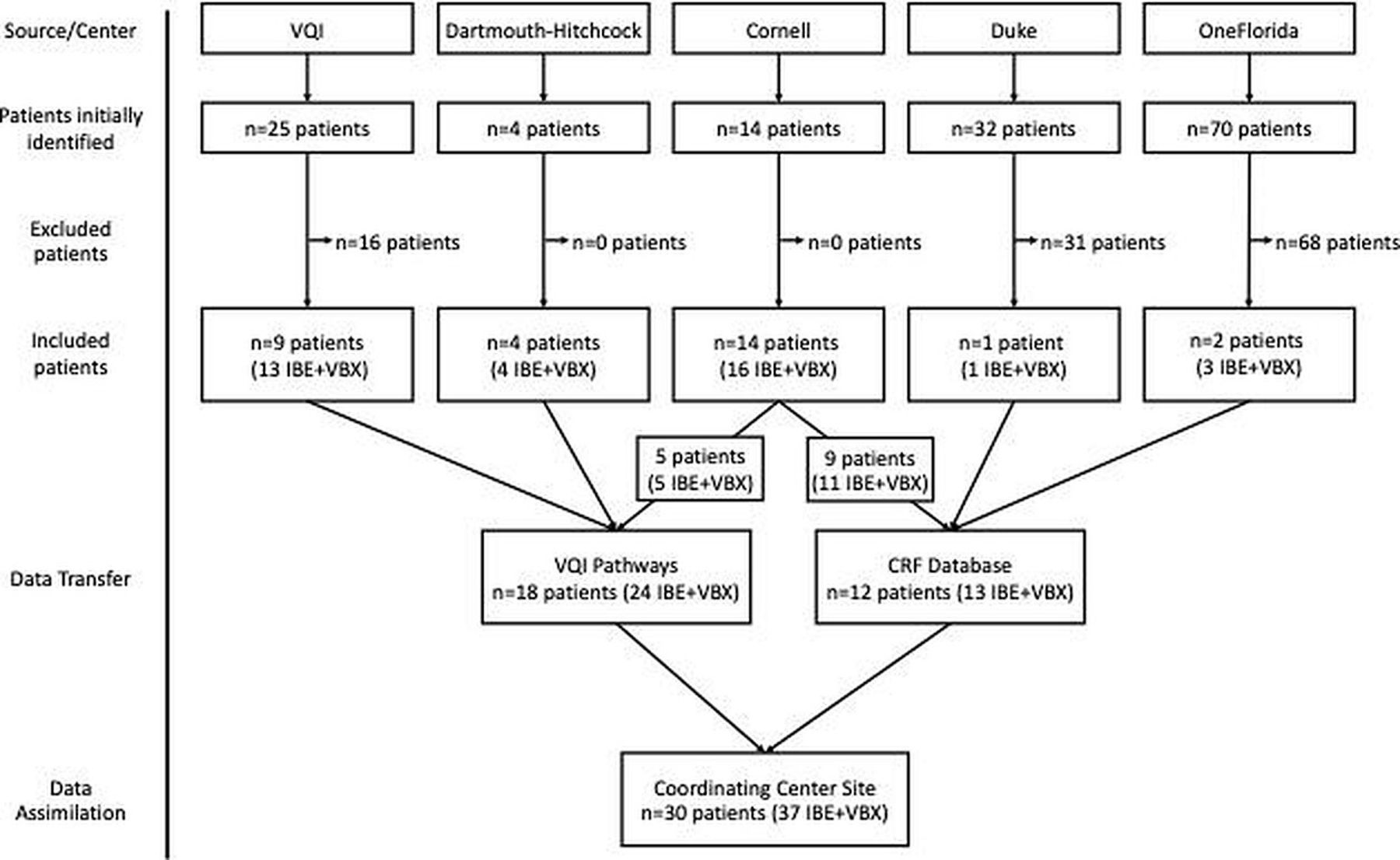
Initial search processes identified 120 cases within the participating centres and 25 cases within the VQI registry (figure 2). Of the potential cases identified within the participating centres, 99 were excluded because IBE +VBX stent graft implantation was not confirmed. Within the VQI registry, 16 cases were excluded because the hashtag variables were not obtained. At the conclusion of the case identification and verification process, a total of 30 patients with 37 IBE +VBX stent graft were identified. Each of the 30 patients and 37 IBE +VBX stent graft were performed in conjunction with an endovascular abdominal aortic aneurysm repair. An additional case in which an IBE was used with a balloon expandable endoprosthesis from another manufacturer deployed in place of the Gore IIC was also identified. Data from each case were successfully transferred to the coordinating centre site via either VQI Pathways or through secure file transfer of the CRF database and merged for final analysis. Figure 2 depicts these case identification results from the VQI registry and each participating site as well as the subsequent data transfer process.
{kind=link}
{kind=link}
Schematic depicting the case identification process and number of cases identified across participating study sites and the Vascular Quality Initiative (VQI). IBE, Iliac Branch Endoprosthesis; VBX, GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis.
Cohort characteristics
The mean age of included patients was 71.6±10.2 years. The cohort was 90% male and 77% white, 10% black, 3% Hispanic and 10% other. Complete demographics are outlined in table 3.
Demographics of cohort with GORE EXCLUDER Iliac Branch Endoprosthesis and GORE VIABAHN VBX balloon expandable endoprosthesis
Intraoperative outcomes
Intraoperative details demonstrated 89% of cases were performed percutaneously, 5% required surgical exposure following failed percutaneous access and 6% required open surgical exposure outright. Mean contrast administration was 130.0±75.3 mL and mean fluoroscopy time was 60.2±28.7 min. Any intraoperative complications were reported in 13.3% (n=4) of the cases, all of which were noted to be endoleaks identified during the case. One endoleak was classified as type II and the remaining three were indeterminate.
Postoperative outcomes
Postoperative details were notable for 43% requiring admission to the ICU postoperatively with a median ICU LOS of 1 day (range: 1–2). Median total LOS was 1 day (IQR: 1–2). There were no postoperative myocardial infarctions, no reported leg embolic events and no reported in-hospital reinterventions. Mean postoperative change in creatinine, defined as the difference between the highest postoperative serum creatinine and the preoperative serum creatinine was −0.40 mg/dL (range: −12.28–0.89 mg/dL). Access site complications were described in 1 of 28 patients, manifesting as a haematoma or pseudoaneurysm. Ultimately, 97% were discharged to home and one patient was discharged to a nursing home or rehabilitation facility. There were no 30-day perioperative deaths.
Discussion
Through this work, we demonstrate the feasibility of identifying and aggregating low-cost real-world medical device data into one registry under the intention of device monitoring and informing regulatory decisions. We identified 30 patients who were treated with 37 implantations of GORE VIABAHN VBX Balloon Expandable Endoprosthesis as a substitute for the internal iliac limb in a GORE EXCLUDER IBE. Demographic and short-term outcomes data for these patients were successfully collected across participating centres and, ultimately, compiled for evaluation. This evaluation demonstrated no postoperative complications including myocardial infarction or leg embolisations, no reported in-hospital reinterventions, and no 30-day perioperative deaths. This work demonstrates the potential to assess and report on short-term outcomes while expanding the types of data available for use in both research and regulatory reporting.
Efforts to expand the types and sources of data used for medical device and pharmaceutical evaluation and monitoring have been put forth by the FDA.8 9 Through these efforts, the Medical Device Epidemiology Network was established in 2010 as a public–private partnership to create a national patient-centred medical device evaluation and surveillance system.10 In 2016, the National Evaluation System for health Technology Coordinating Centre (NESTcc) was established in order to address the lack of high-quality, near real-time, and low-cost evidence regarding medical devices.8 11 Since their inception, these organisations have supported and acknowledged the development and use of new medical device evidence generation and evaluation.12–15
In addition to this test case, NESTcc has funded additional work exploring the feasibility of using real-world data sources as a means of exploring off-label medical device uses.16 These test cases pertain to an array of medical devices and include cardiac ablation catheters, soft tissue thermal ablation devices, and cardiac devices used in the treatment of paediatric patients with congenital heart diseases.16 Through the support of NESTcc, these projects, including ours, are exploring the ability to capture necessary data, evaluate if the data are of appropriate quality, and if there is a sufficient sample size available to support future regulatory submissions. If successful, these test cases may outline data collection mechanisms which may be used to expand the indications for use and inform physicians about treatment options for patients.
Through these mechanisms, realistic generation of data which could be used to inform regulatory decisions or support indication expansions would require longer-term follow-up data. The data collected through this work included procedural, predischarge, and 30-day mortality events. Thirty-day outcomes, such as these, can be considered reflective of procedural safety. While this is informative, regulatory authorities will often require data demonstrating durability of the treatment past this time period in order to make their assessments. The ability to collect follow-up data to combine with periprocedural data represents a practical hurdle for this data collection mechanism. Future efforts should include outcome events beyond this window.
This work has limitations. As a feasibility study, the final sample size from which outcomes were derived is limited and may not represent the larger experience with off-label IBE+VBX stent graft use. While certainly feasible, as demonstrated by this study, gathering and assimilating real-world evidence under the intention of device monitoring does face challenges and has limitations. First, data is siloed within health systems where it is catalogued and stored in unique ways. As a result, each participating site had to develop a unique case identification process tailored to their specific data organisational scheme. The number of potential cases identified by each strategy was variable and likely stems from the unique nature of each data source and the resultant search strategy. Ultimately, the ability of each of these unique approaches to identify the true number of cases at each site is unknown. Second, the ability to perform centralised data auditing was limited. Data collection was performed separately at each individual site and, once collected, transferred to the coordinating centre. While efforts were made to establish clear variable definitions and each site conducted individual data audits, the compiled data could not be cross-referenced with the electronic medical record to ensure accuracy and reliability. Additionally, the variables included were built on those routinely collected by the VQI. While robust, these variables do not allow for the same granularity as chart review analyses. For example, the VQI limits the number of devices listed as implanted in the iliac to three. Should more devices have been implanted, they would not be captured in the current VQI framework. Similarly, using the VQI modules as they exist now presents an inherent limitation in long-term follow-up and the data available which would be necessary to evaluate device efficacy and durability. Finally, the data transfer process required mirroring DUAs between each participating site and the coordinating centre. Navigating these data permissions was complex but an essential aspect of collaborative work such as this. These challenges and limitations pose as areas for future innovation and improvement to allow for more robust, widespread and efficient data collection.
In conclusion, we have demonstrated that real-world evidence, as it pertains to an unapproved combination of endovascular devices (IBE+VBX stent graft), can be identified, gathered, and integrated with the intention of evaluating short term outcomes. This success opens the possibility of using such an approach, applied more broadly and with efforts to address the limitations unveiled through this work, as a means of generating data for device monitoring, submission to regulatory agencies, or for consideration in indications expansions and approval.
Data availability statement
No data are available. Data contains PHI and is governed by bilateral data sharing agreements between the Coordinating Center Site and Duke and OneFlorida, and pre-existing agreements with the Society for Vascular Surgery Patient Safety Organisation, and AHRQ listed patient safety organisation. Due to the small sample size, data can not be shared.
Ethics statements
Patient consent for publication
Ethics approval
This study underwent local institutional review board approval at each participating centre (Dartmouth-Hitchcock Medical Center Committee for the Protection of Human Subjects #00031488; Weill Cornell Medicine Human Research Protection ProgramProgramme #1806019366; University of Florida Institutional Review Board #201900458; DukeHealth Institutional Review Board #00101721).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jaaronb_md, @JialinMao, @Artsytwits, @DartmthSurgHSR
Contributors JAB, conception/design of the work; acquisition and analysis; manuscript drafting; final edits/approval; guarantor. MAE: conception/design of the work; acquisition and analysis; manuscript drafting; final edits/approval. KM: conception/design of the work; acquisition and analysis; manuscript drafting; final edits/approval. SA: conception/design of the work; acquisition and analysis; final edits/approval. EG: conception/design of the work; acquisition and analysis; final edits/approval. JNW: conception/design of the work; final edits/approval. NK: conception/design of the work; acquisition and analysis; final edits/approval. JM: conception/design of the work; acquisition and analysis; final edits/approval. DPK: acquisition and analysis; final edits/approval. BDS: acquisition and analysis; final edits/approval. DS: acquisition and analysis; final edits/approval. TA: conception/design of the work; manuscript drafting; final edits/approval. RZ: conception/design of the work; manuscript drafting; final edits/approval. SV: conception/design of the work; acquisition and analysis; final edits/approval. EAS: conception/design of the work; acquisition and analysis; final edits/approval. AS: conception/design of the work; acquisition and analysis; manuscript drafting; final edits/approval. PG: conception/design of the work; acquisition and analysis; manuscript drafting; final edits/approval; guarantor.
Funding The National Evaluation System for Health Technology Coordinating CenterCentre (NESTcc; https://nestcc.org) selected this test case under grant number R1-TC1. NESTcc supports timely, reliable and cost-effective evidence development for medical device evaluation.
Competing interests W. L. Gore & Associates, manufacturer of the GORE EXCLUDER Iliac Branch Endoprosthesis and GORE VIABAHN VBX Balloon Expandable Endoprosthesis,participated in project conceptualisation, design, analysis and manuscript preparation.Please hold this paper and do not publish it until one or two commentaries are received. Art Sedrakyan is an Editor in Chief and Jialin Mao and Philip P. Goodney are Associate Editors.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.