Article Text

Statistics from Altmetric.com
- device removal
- device surveillance
- orthopedic devices
- maxillofacial prosthesis implantation
- device safety
Bioabsorbable plates and screws (BPS) are now widely used as a well-established internal fixation method for various osteosynthetic surgeries, such as fixation of fractures or osteotomies. One of the BPS’s main advantages is that surgical removal is unnecessary since they are ostensibly fully absorbed over time.1 2 In fact, to date there have been few reports available focusing on surgical removal of BPS. For example, one large series (n=1883 patients) of absorbable plate and screw fixations in pediatric craniofacial surgery confirmed that none of the devices required surgical removal.3 Another review article, assessing 19 papers consisting of 438 patients, reported 8–10 cases of implant removal.4
In the premarket evaluation by the Pharmaceuticals and Medical Devices Agency (PMDA) of Japan, the effectiveness and safety of BPS have been evaluated in clinical trials which consist of a small number of study subjects with limited follow-up. Still, it is difficult to identify rare adverse events (AEs) before approval, particularly in the late follow-up phase. The PMDA of Japan has adverse events and infections reporting system for medical devices. Marketing authorization holders (MAHs) are obligated to submit an AE report to the PMDA under the provision of the PMD Act (ie, Law on Securing Quality, Efficacy, and Safety of Products, Including Pharmaceuticals and Medical Devices). The limitations of this system is that if the MAH does not capture the events, then these will not be reported to the PMDA. Hence, the real number of events is likely to be much higher than reported. It is also impossible to identify the denominator (total patient-years of the device used) so that the exact incidence of the events cannot be calculated. Despite these limitations, the AE reporting system remains critically important for detection of rare events in the late follow-up phase.
To identify and analyze late BPS removal, the AE database of PMDA was searched from October 2003 to July 2016, and a total of 162 cases of BPS removal were identified. Of these, 89 (54.9%) were male and 53 (32.7%) were female, and for 20 (12.3%) cases the gender was unknown. The median age was 30 years (IQR, 43–20 years), and age was not known in 41 (25.3%) cases.
Indications for original surgery
The main reason to use BPS in the original surgery was trauma in 96 (59.3%) cases (87 cases for maxillofacial fracture, 9 cases for limb injury). Other surgeries included bone fixation secondary to thoracotomy, open heart surgery or craniotomy in 15 (9.3%) cases; fixation of congenital disease in 13 (8.0%) cases; jaw deformity in 12 (7.4%) cases; degenerative disease in 7 (4.3%) cases; tumor in 2 (1.2%) cases; and unknown in 17 (10.5%) cases.
AE timing and type
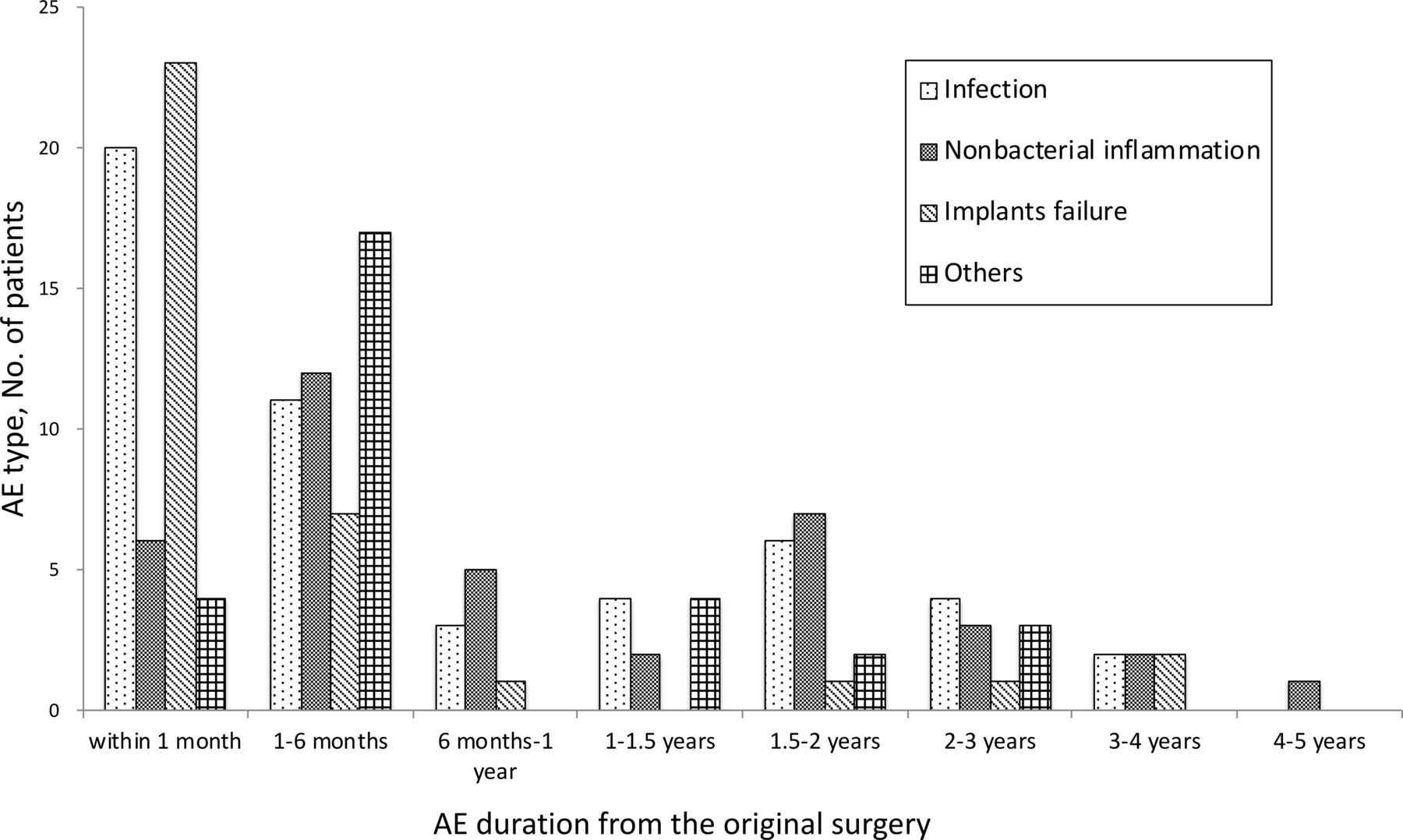
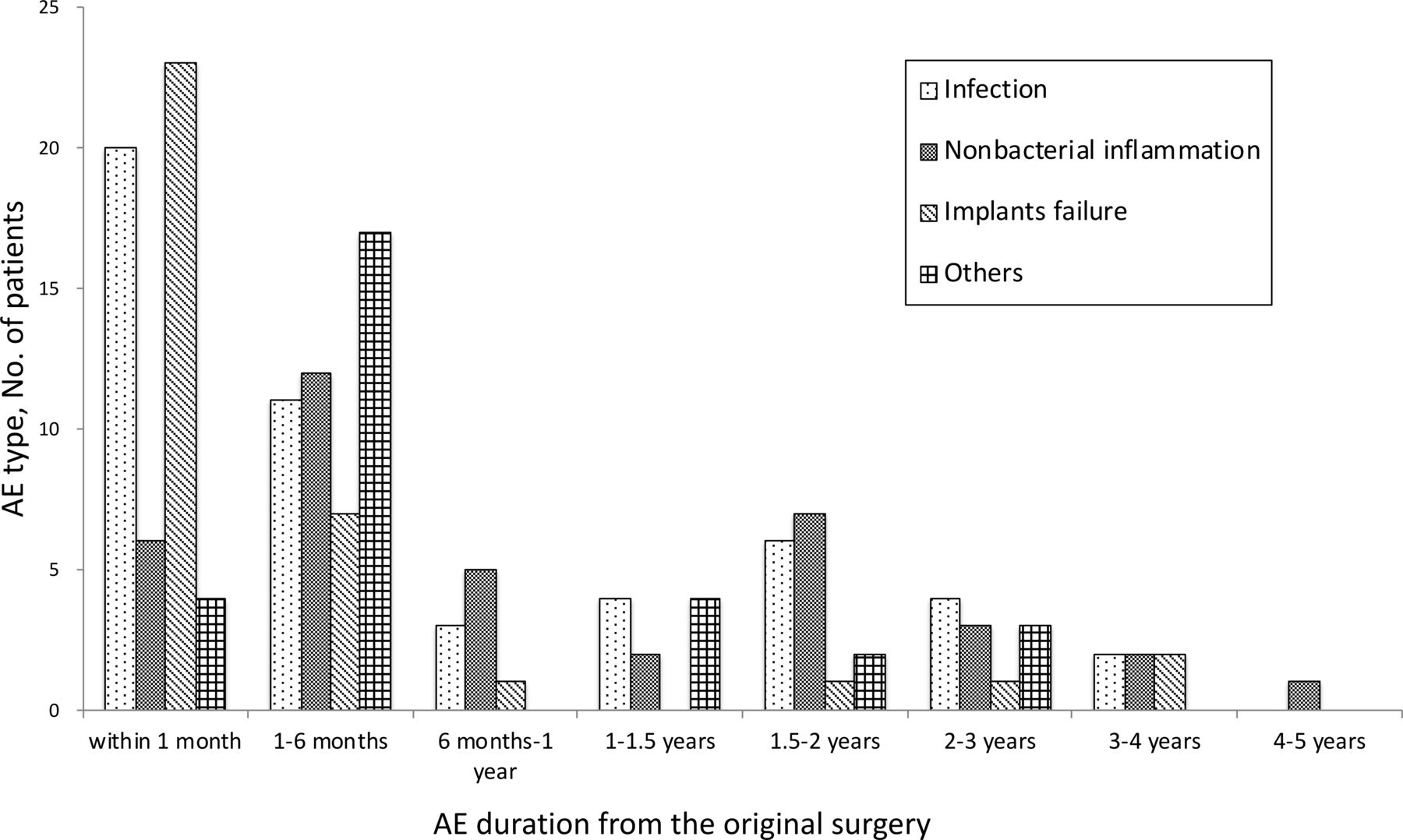
The intervals between the original surgery and AE development and the type of AE are shown in figure 1. One hundred cases (61.7%) occurred within 6 months (ie, 53 cases within 1 month and 47 cases between 1 and 6 months), while 53 (32.7%) cases occurred after 6 months. AEs were constantly reported up to 4.5 years. The main reason for surgical removal within 1 month was either infection or implant failure. In contrast, surgical removal after 6 months was mostly due to either late infection or non-bacterial inflammatory reaction (figure 1).
{kind=link}
Types of AE and time of onset of AE from the original surgery. A total of 53 cases occurred within 1 month after BPS implantation, and 47 cases from 1 to 6 months post-implantation. Late removal after 6 months was required in 53 (32.7%) cases, mainly due to either late infection (19 cases, 11.7%) or non-bacterial inflammation (20 cases, 12.3%). Infections within 1 month were the most frequent in 20 (39.2%) cases. However, delayed infections after 6 months were also reported in 19 (37.3%) cases. Non-bacterial inflammations were the most frequent (20 cases, 50%) after 6 months, whereas implant failures were the most frequent (23 cases, 57.5%) within 1 month. An increase in AE was observed after 1.5–2 years of implantation. The longest duration post-BPS implantation was found at 4 years and 6 months. AE, adverse event; BPS, bioabsorbable plates and screws.
Materials used in implants
The materials used in eight BPS items, consisting of three bioabsorbable plates and five bioabsorbable screws, were as follows: three items consist of poly-L-lactic acid (PLLA); four items of unsintered hydroxyapatite and PLLA; and one item of copolymers of PLLA and polyglycolic acid. There was no significant difference in event occurrence by implant materials.
The present aggregated results lead us to focus on the following several findings. First, late AEs 6 months post-implantation accounted for one-third of them. Second, it is important to note that late phase infection, after 6 months, occurred in 19 cases, which is nearly equal to 20 cases in the acute infection phase, within 1 month. Third, most cases of surgical removal followed BPS implantation in cranial or maxillofacial surgery, which requires reflection. Finally, although speed of absorption differed among the different BPS materials, foreign body reactions are known to occur during a later follow-up phase, approximately between 6 months and 5 years after surgery,1 4 5 as observed in the study.
Given the results of our study we would like to send the message to surgeons who use BPS that BPS might require surgical removal during a later follow-up period, even after 6 months and up to 4.5 years. Continuous and careful follow-up, especially monitoring for possible infections and non-bacterial inflammations, should be considered as needed. Additionally, patients treated with BPS must be fully informed about the potential AEs that may occur before BPS’s complete degradation, as well as the possibility of surgical removal.
Footnotes
Contributors TK and NH designed the study, and TK wrote the initial draft of the manuscript. TK, NH, SM, and KK contributed to analysis and interpretation of data, and assisted in the preparation of the manuscript. All other authors have contributed to data collection and interpretation, and critically reviewed the manuscript. All authors approved the final version of the manuscript, and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views and opinions expressed in the manuscript are the authors’ and do not necessarily reflect the official view of the PMDA.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the ethical committee of PMDA .
Provenance and peer review Not commissioned; externally peer reviewed.